Effects of Biofeedback-Aided Relaxation on the Psychological Stress Symptoms of College Students
Author: Richard J. Fehring
Author: The purpose of this study was to compare the effects of Benson's relaxation technique (BRT) with Benson's technique augmented with GSR biofeedback (i.e., biofeedback-aided relaxation, BAR) on the psychological stress symptoms of well college students. Seventy-eight normotensive college students were randomly assigned to one of three groups: the BRT group, the BAR group, and a control group. The BRT and BAR students were asked to practice their respective relaxation technique daily for an eight-week period. Pre-and postintervention, all subjects were administered a state-anxiety inventory and a profile-of-mood state (POMS) test. Posttest analysis indicated that the BAR group had significantly lower state anxiety and POMS than the BRT and control groups (p < 0.05). It was evident from the results that BAR did augment BRT in lowering psychological stress symptoms. Part of the effectiveness was due to the expectation of relief on the part of the BAR group. It was recommended that nurses study the effects of BAR in clinical settings.
Stress and the management of stress are very much an integral part of health and well-being today. In recent years, many papers, books, and journals have been written on the subject and multiple approaches have been advocated to manage it. This recent interest in stress stems not only from the apparent pace and change of a modern life-style but also from various studies supporting the age-old theory that life's stresses can lead to many health problems. The stress-disease theory-particularly relevant in today's society-attributes the majority of its disease patterns not to germs, inadequate sanitation, or poor living conditions but rather to the stress and pace of a modern technological society (Sutterley, 1979).
Stress can be defined in terms of environmental situations that disrupt a person's preferred style of living, resulting in a state of hyperpsychophysiological arousal (Benson, 1975, 1977). It is believed that stress becomes maladaptive when this state of hyperarousal continues too long, occurs too frequently, deteriorates physical and mental performance, or results in a stress-related health problem (Budzynski, 1978). Maladaptive stress has been implicated as a contributing cause to many of today's health problems including heart disease, hypertension, and cancer. College students experience an exceptional amount of stress (Marx, 1974; Garrity, 1977). They have to deal not only with the social transition from high school to university, but also with personal concerns of self-review, identity, sexual attitudes, and philosophical and social values. Likewise, long study hours, deadlines, examinations, noisy dorms, lack of sleep, and poor eating habits all contribute to a student's stressful life.
There are now indications that many of the major stress disorders (such as coronary heart disease) begin at a young age (Friedman & Roseman, 1974). Therefore, it seems reasonable to conclude that if college students could learn to manage stress in a healthy way, perhaps they could prevent stress-related disorders. Relaxation and biofeedback techniques are purported to be effective in helping people to manage stress and to reduce stress-related symptoms. The purpose of this study, therefore, was to compare the effectiveness of a simple relaxation technique (Benson's relaxation technique) with the same relaxation technique augmented with biofeedback on the psychological stress symptoms of college students.
Background
Benson (1975) studied various techniques that produce what he calls the "relaxation response": a response that exhibits a calming psychophysiological state opposite to the hyperarousal state produced by stress. Benson (1977) stated that practicing these techniques for 10 to 20 minutes twice a day should help people lower their psychophysiological stress levels and protect against the effects of stress.
Many studies have investigated the effects of various relaxation techniques (Tarler-Benlolo, 1978). However, only a few have investigated the effects of Benson's relaxation technique. In fact, a study by Peters, Benson, and Porter (1977) was the first investigation that used a control group, long-term intervention, and a healthy "normotensive" population. There are still many questions concerning Benson's relaxation technique: For example, how effective it is, how often it needs to be practiced, how compliant people are in using it, and whether the technique is any more effective than just sitting quietly in a chair. Some researchers believe that relaxation techniques such as Benson's are no more effective than teaching a person how to catnap (Brown, 1977). Catnapping, however, might be very beneficial in helping to prevent stress-related disorders. One problem with Benson's technique is that it does not give the person who practices it any immediate and continuous information as to the level of relaxation that he or she is experiencing or, for that matter, if the person is actually relaxing at all.
The GSR II® (made by Thought Technology) is a small hand-held instrument that records galvanic skin resistance (GSR). Galvanic skin resistance is related to the physiological arousal level of an individual (Fuller, 1978). As a person becomes physiologically aroused, skin resistance decreases, and as a person relaxes, skin resistance increases. The GSR II biofeedback monitor reflects this activity with an audible tone that decreases or increases according to the level of skin resistance. This simple device enables a person to have some idea of a level of arousal and helps to sensitize a person to the messages given from the skin. Very little research, however, has been conducted to determine the effectiveness of these home-practice devices.
The following terms were used in this study:
- BRT-Benson's Relaxation Technique: A mental device that results in a relaxed psychophysiological response.
- BAR -Biofeedback-Aided Relaxation: The use of biofeedback instrumentation in conjunction with a relaxation technique in order to receive immediate information about the level of psychophysiological relaxation being achieved (Fuller, 1977).
- Psychological Stress Symptoms: Psychological stress symptoms can be generally described as perceived mental and physical manifestations of stress. Examples are anxiety, tension, fatigue, and irritability.
Psychological stress symptoms were measured by the State Form (X-1) of the State Trait Anxiety Inventory (STAI) developed by Spielberger, Gorsuch, and Lushene (1970) and by the Profile of Mood States (POMS) test developed by McNair, Lorr, and Droppleman (1971).
The A-State Form of the STAI was designed to measure respondent's anxiety as perceived at that moment. Alpha reliability coefficients for the A-State scale range from .83 to .92 (Spielberger et aI., 1970). Validity for the STAI has been demonstrated in a wide variety of studies. The A-State scale has 20 items, each based on a 4-point scale that indicates high to low anxiety or low to high anxiety according to the direction the items are stated (e.g., "I am tense" or "I feel pleasant"). The range of possible scores varies from 20 to 80.
The POMS is a factor ally derived inventory of 65-point adjectives that measure six identifiable mood or affective states:
tension-anxiety, depression, anger, vigor, fatigue, and confusion. Validity and reliability for the POMS have been reported by McNair et aI. (1971). A score for each of the individual mood states may be obtained by summing the responses obtained for the adjectives defining the factor. Each adjective is ranked by a Likert-type scale. A total mood disturbance score is obtained by summing the scores (with vigor weighted negatively) on the six primary mood states.
Internal consistency for all the factors of the POMS reaches a correlation of .90 or above (McNair et aI., 1971). Test-retest reliability ranges from .65 for vigor to .74 for depression. K-R reliability ranges from .84 to .95.
Factoral validity was obtained through six factor analytical replications (McNair et aI., 1971). Predictive and construct validity were obtained from four areas of research: (1) brief psychotherapy studies, (2) controlled outpatient drug trials, (3) studies of responses to emotion-inducing conditions, and (4) studies of concurrent validity coefficients and other POMS correlates.
Hypotheses
The following hypotheses formulated for this study were:
- College students who practice BAR on a daily basis will have lower state anxiety than those students who practice BRT or no relaxation technique at all.
- College students who practice BAR on a daily basis will have lower POMS scores than those students who practice BRT or no relaxation technique at all.
Method
A three-group experimental design was employed. The three groups consisted of subjects randomly assigned to one of three treatment conditions: Group A1-BRT, Group A2-BAR, and Group A3-controI. Subjects in all three groups had their psychological stress symptoms measured before and after an eight-week experimental period.
The subjects were all college students between the ages of 18 and 35. Each of the subjects (1) had a blood pressure below 140/90 mm Hg, (2) had never regularly practiced any relaxation technique, and (3) was not being treated for any major health problem.
To obtain subjects for this investigation, a booth was set up at various sites on a university campus. The booth displayed biofeedback monitors, relaxation tapes, books on stress management, and a sign that asked for students to participate in stress management research and to learn relaxation and biofeedback techniques. Potential subjects had their blood pressures taken by the researcher. Students who met the blood-pressure criteria signed a formal volunteer agreement form and were given appointments to have their psychological stress symptoms measured.
Ninety-eight students agreed to participate in the research investigation, but only 90 subjects returned. After the prestress measurement session, the 90 subjects were randomly assigned to one of the three groups. Seventy-eight of the original 90 subjects remained for the length of the investigation: 26 subjects in each group. Of these 78 subjects, 17 were male and 61 female. Groups A1 and A2 each had 7 males and 19 females and Group A3 had 3 males and 23 females. (The majority of subjects were female because subjects were first selected from the School of Nursing.) The average age of the 78 subjects was 22.8 years. The average age in Group A1 was 23.0 years, A2, 21.8 years, and A3, 23.7 years.
The subjects were randomly assigned to the groups and given an appointment to have their stress levels measured at the University Nurse Health Clinic (UNHC). When the subjects reported to the clinic, they were seated in comfortable chairs and administered the STAI and POMS psychological tests. The control subjects were then given appointments to return to the UNHC in eight weeks. The subjects in Groups A1 and A2 were given appointments to return in one week. At this appointment, the subjects in Group A2 met in groups of two to five and were given a GSR II recorder, an instruction book on how to use the recorder, and a tape cassette that explained the principles and use of the GSR II biofeedback instrument.
The ten-minute instruction tape was played to the subjects at the beginning of the sessions. They were then given a copy of the following instructions, which entail a combination of directions for use of the GSR II and Benson's relaxation technique.
- Sit quietly in a comfortable position.
- Place your GSR II recorder in your left hand and adjust the tone to a medium pitch.
- Close your eyes.
- Deeply relax all your muscles. Begin with your feet.
- Breathe through your nose and become aware of your breathing. As you breathe, focus on the tone of the GSR recorder and try to passively lower the tone. Continue to breathe easily and naturally.
- Continue for 10 to 12 minutes. When you finish, sit quietly for several minutes. Do not stand for several minutes.
- Maintain a passive attitude while relaxing and permit relaxation to occur at its own pace. When disturbing thoughts occur, try to ignore them by not dwelling on them and return to focusing on the tone of the recorder. Practice the technique at least once a day, but not within two hours of any meal, as the digestive process seems to interfere with elicitation of the relaxation response.
After reading the instructions, these subjects practiced relaxing with the GSR II recorders for 10-12 minutes. They were then asked to practice BAR at least once a day for the next eight weeks and to record the time and date they practiced the technique in a small notebook provided to them.
The subjects in Group A1 also met in groups of two to five and were given a copy of the instructions for Benson's relaxation technique. These instructions were similar to instructions for BAR except that the subjects were asked to silently repeat the word "one" instead of focusing on the tone of the biofeedback recorder. After the relaxation technique was read, the subjects practiced the instructions for 10 to 12 minutes. Like the subjects in Group A2, they were asked to practice their relaxation technique once daily for the next eight weeks and to record the time and date of their home-practice sessions. Subjects in both Groups A1 and A2 were also given five small stick-on red dots to place on objects in their environment. These dots were to remind them to periodically check their bodies for tension and to use their respective relaxation technique to decrease this tension. These subjects were then given appointments to return to the UNHC in eight weeks for poststress measurements.
At the end of the eight-week practice period, the 78 subjects remaining in the experiment again took the STAI and POMS tests.
To test if there was a statistical difference in the subject's psychological stress levels prior to the intervention of the relaxation techniques, a one-way analysis of variance (ANOVA) was performed on the scores of STAI and POMS. After an eight-week period of intervention, another one-way ANOV A was done to find differences between the STAI and POMS scores of the three treatment groups. Level of significance was set at p < 0.05.
Results
STAI: There was no statistical difference among the premean state-anxiety scores of the three treatment groups, with F (2, 75) = 0.18 and p = 0.84 (Table 1). Therefore, the pretest data established that the three treatment groups had statistically equivalent state-anxiety levels prior to intervention.
POMS: No statistical difference was found among the premean POMS scores of the three groups, with F (2, 75) = 1.28 and p = 0.28 (Table 1). A separate univariate F was also generated for each of the six adjective scales of the POMS (Table 2). Like the total mood disturbance scores (total POMS), the separate adjective mean scores did not show any significant differences. Again, the pretest data supported the lack of difference of the groups in total POMS and separate POMS adjective scores.
Although there was no statistical difference among the three groups in regard to the STAI and POMS scores, the biofeedback group's mean POMS score was nearly 14 points lower then the other two groups. In addition, the Bartlett-Fox F test to check homogeneity of variance showed equal variances for the STAI scores but not the POMS, with F = 3.38 and p = 0.03. There were also large standard deviations for the scores of the three psychological tests (Tables 1 and 2). This was due to the large range of scores and to a platykurtotic distribution. However, because the three groups had an equal number of subjects, violations of normality and homogeneity of variance should not affect the final analysis of variance (Dayton, 1970).
Hypothesis I was supported. A statistical difference was found among the mean state-anxiety scores of the three groups, with F (2, 75) = 3.48 and p = 0.04 (Table 3). Duncan post-hoc analysis of the state-anxiety scores found the BAR group to have significantly lower state anxiety than both the BRT and control groups (p < 0.05, Table 4). There was no significant difference between the state-anxiety scores of the BRT and control groups.
Hypothesis II was also supported. A univariate F (2, 75) = 4.09 indicated a significant difference among groups at p = 0.02 (Table 3). Post-hoc analysis revealed that the BAR group had significantly lower total mean POMS scores than both the BRT and control groups (p < 0.05). There was no difference in the mean POMS scores of the BRT and control groups.
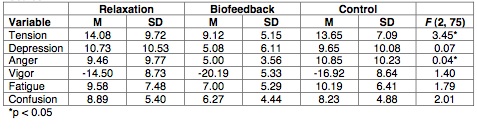
Individual univariate F's were also calculated for the six posttest mean adjective-scale scores in order to see which were contributing to the overall total POMS difference (Table 5). Of these six scores, only the tension-anxiety and the anger-hostility mean scores showed any statistical difference. Subsequent post-hoc analysis showed that the BAR group only had significantly lower tension-anxiety scores than both the BRT and control groups (Table 4). There was no statistical difference between the scores of the relaxation and control groups on all six scales.
Discussion
These results are somewhat consistent with past findings in that biofeedback and cognitive relaxation techniques (such as BRT) have-been consistent in decreasing self-reported anxiety and other stress-related mood states (Tarler-Benlolo, 1978). Past studies are inconsistent, however, in reporting the comparative effectiveness between biofeedback and relaxation techniques. The results show BAR to be clearly more effective than BRT in that the BAR group had lower anxiety and POMS scores.
There are a number of possible reasons to account for the different results between the two techniques and the control. The first reason is the difference in the amount of use of the respective techniques. A difference would be expected if one group practiced their respective relaxation technique more than the other. The study by Ferguson and Gowan (1976) demonstrated that experienced TM meditators were able to lower their state anxiety more than the less experienced meditators. This practice difference could explain the higher state anxiety and POMS scores of the control group. The control group did not practice relaxation over the eight-week period. This, however, would not explain the higher state anxiety and POMS levels for the relaxation group. Compliance data did not reveal any difference in home-practice sessions between the BAR and BRT groups. The mean number of practice sessions (per week) for the BRT group was 4.4 and for the BAR group, 4.9. An independent t = 1.16 did not reveal a significant difference in sessions between the groups.
Because compliance data was taken from self-reports of subjects, interpretation must be limited. No attempt was made to check validity or reliability. Besides basic compliance in practicing BAR or BRT, whether the individual subjects actually achieved a relaxation response must also be considered. The effectiveness of a biofeedback or relaxation technique can only be determined if a level of relaxation actually has been accomplished (Taub, 1982). Whether a subject is effective in achieving relaxation with BAR or BRT would be difficult to .determine unless the subject was attached to monitoring devices. This would preclude home practice. This study, however, could have had the subjects in the BAR group record each time they were able to decrease or shut off the tone on their GSR recorder. Both groups could also have reported subjective experiences of relaxation and/or pre- and post-heart rates. The differences in the anxiety, POMS, and tension levels of the BAR and BRT groups might be due to the BAR group's better sense of relaxation with the GSR monitor. It would be recommended in further studies to determine the frequency of practice as well as the achieved levels of relaxation.
A final reason that the POMS scores and anxiety levels were lower for the BAR group than the BRT and control groups could be that the BAR group may have had greater expectations of relief (i.e., the placebo or novelty effect). Biofeedback has become popular in the past ten years as a remedy for stress and anxiety. The subjects in the BAR group might have reflected this. To control for this expectation, a group with a placebo technique could have been designed for this study. The BRT technique, however, was also taught as a method to relieve stress. Therefore, subjects in the BRT group should also have reflected an expectational factor. The results indicated that they did not.
Finally, the results of this study were similar to the study by Townsend, House, and Addrio (1975), who found biofeedback to be more effective in reducing total POMS and state anxiety than group therapy. Townsend's et al. study did not report the breakdown results of the six adjective scales of the total POMS.
It would have been interesting to make a comparison of the six adjective-breakdown results with Townsend's et al. (1975) study because this present study only demonstrated significant findings with the tension and anger subscales of the total POMS. All the other scales (i.e., vigor, fatigue, confusion, and depression), even though not significantly different, did contribute to the total POMS difference by either being lower or higher in the appropriate direction. For example, the vigor scores of the BAR group were 1.9 to 2.3 points higher than the BRT and control groups, and the depression scores were 4.5 to 5.6 points lower. Further studies on the effects of BAR (and other biofeedback techniques) on the total POMS and comparison of results of the six subscales are recommended. It would also be interesting to see if biofeedback therapy consistently decreased only the tension and anger subscales of the total POMS.
Implications for Nursing
The implication that these findings for nursing practice is that BAR is a simple cognitive technique that nurses could easily teach clients (healthy or sick) in order to help them to prevent or decrease stress symptoms of a psychological nature. Moreover, BAR is a technique that could be particularly useful to the patient in the hospital setting. There are many situations that occur while an individual is hospitalized that precipitate both cognitive and somatic stress symptoms. These symptoms are often detrimental to recovery and rehabilitation. Stressful situations in which BAR may be applicable are: before and after diagnostic tests (such as cardiac catheterization), before and after surgery, during childbirth, during recovery from a myocardial infarction, after the stress of an intensive care setting, and while being weaned from a mechanical respirator. It is recommended that nurses do further research to investigate the effects of BAR on stress symptoms' in clinical situations.
References
- Benson, H. The relaxation response. New York: William Morrow & Co., 1975.
- Benson, H. Systematic hypertension and the relaxation response. New England Journal of Medicine, 1977, 20, 1152-1156.
- Brown, B. Stress and the art of biofeedback. New York: Harper & Row, 1977.
- Budzynski, T H. Biofeedback applications to stress-related disorders. International Review of Applied Psychology, October 1978, 27, 73-79.
- Dayton, C. M. The design of educational experiments. New York: McGraw-Hill Book Co., 1970.
- Ferguson, P., & Gowan, J. T.M:Some preliminary findings. Journal of Humanistic Psychology, Summer 1976, 16, 51-60.
- Friedman, M., & Roseman, R. H. Type A behavior and your heart. New York: Alfred A. Knopf, 1974.
- Fuller, G. D. Biofeedback: methods and procedures in clinical practice. San Francisco: Biofeedback Press, 1977.
- Garrity, T. F., Grant, W. S., & Marx, M. B. The relationship of personality, life change, psychophysiological strain and health status in a college population. Social Science and Medicine, 1977, 11, 257-262.
- Marx, M. B., Garrity, T. F., & Bowers, F. R. The influence of recent life experience on the health of college freshman. Journal of Psychosomatic Research, 1975, 19, 87-98.
- McNair, D. M., Lorr, M., & Droppleman, L. F. Profile of mood states. San Diego: Educational and Industrial Testing Service, 1971.
- Peters, R. K., Benson, H., & Porter, D. Daily relaxation response breaks in a working population: Part 1. Effects on self-reported measures of health, performance, and well-being. American Journal of Public Health, 1977, 67, 946-953.
- Spielberger, C D., Gorsuch, R. L., & Lushene, R. E. STAI manual for the state-trait anxiety inventory. Palo Alto, Calif.: Consulting Psychologists Press, 1970.
- Sutterley, D. S. Stress and health: a survey of self-regulation modalities. Topics in Clinical Nursing, April 1979, 1, 1-30.
- Tarler-Benlolo, L. The role of relaxation in biofeedback training: a critical review of the literature. Psychological Bulletin, 1978, 85, 727-755.
- Taub, E. Current status of biofeedback and future directions. Paper presented at the annual meeting of the Society of Behavioral Medicine, Chicago: March 5, 1982.
- Townsend, R. E., House, J. R., & Addrio, D. A. A comparison of biofeedback-mediated relaxation and group therapy in the treatment of chronic anxiety. American Journal of Psychiatry, 1975, 132, 598-601.
Note
Richard J. Fehring, DNSc, RN, is an assistant professor at Marquette University College of Nursing and a part-time staff nurse at St. Anthony Hospital, Milwaukee, WI.
Appendix
Table 1: Pretest Means (M), Standard Deviations (SD), and Univariate F's for the State and POMS Scores
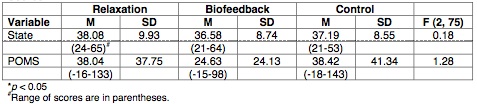
Table 2: Pretest Means, Standard Deviations, and Univariate F's for the Six Adjective Scales of the POMS
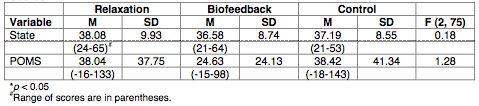
Table 3: Posttest Means, Standard Deviations, and Univariate F's for the State and POMS Scores
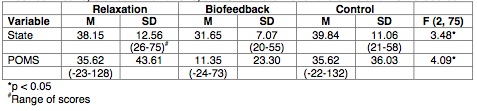
Table 4: Duncan Post-Hoc-Analysis Results of State Anxiety, POMS, and Tension Scores
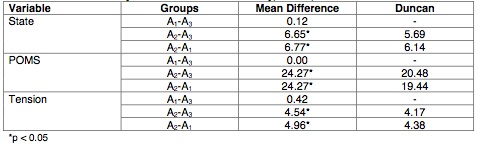
Table 5: Posttest Means, Standard Deviations, and Univariate F's for the Six POMS Adjective Scales
Article copyrights are held solely by author.
[ Japan-Lifeissues.net ] [ OMI Japan/Korea ]